For the use only of a Registered Medical Practitioner or a Hospital or a Laboratory
Metnylprednisolone Acetate Injectable Suspension USP
DEPO-MEDROL™
STERILE AQUEOUS SUSPENSION
Composition
DEPO-MEDROL Sterile aqueous suspension 40 mg per ml Each ml contains.
Metnylprednisolone Acetate USP 40 mg - Polyethylene glycol 3350 - Sodium chloride - Myristyl-gamrra-picolinium chloride 0 2 mg - Water for injection,
Forms, ways of administration and packages
FORM: sterile aqueous suspension for single use
WAYS OF ADMINISTRATION
- Intramuscular
- lntra-articular, periarticular intranasal or soft tissues
- Inlralesional
- Intrarectal instillation
DEPO-MEDROL is contra-indicated for IV. administration DEPO-MEDROL is not recommended for intrathecal epidural intranasal intra-ocular or any other unapproved route ot administration
(see ADVERSE REACTIONS
reported from non recommended routes of administration)
PACKAGES
DEPO-MEDROL Sterile aqueous suspension 40 mg per ml:
-1 ml vial
-2 ml syringe
- 2 ml vial
- 5 ml vial
Properties
DEPO-MEDROL is a sterile aqueous suspension of the synthetic glucocorticoid methylprednisolone acetate. It has a strong and prolonged anti-inflammatory, immunosuppressive and anti-allergic activity
DEPO-MEDROL can be administered I.M for a prolonged systemic activity as well as in situ for a local treatment The prolonged activity of DEPO-MEDROL is explained by the slow release of the active substance
PHARMACODYNAMICS
Methylprednisolone acetate has the general properties of the glucocorticoid methylprednisolone but is less soluble and less readily metabolised which explains its prolonged activity.
Glucocorticoids diffuse across cell membranes and complex with specific cytoplasmic receptors These complexes then enter the cell nucleus, bind to DNA (chromatin), and stimulate transcription of mRNA and subsequent protein synthesis of various enzymes thought to be ultimately responsible tor the numerous effects after systemic use. Glucocorticoids not only have an important influence on inflammatory and immune processes, but also aflect the carbohydrate, protein and fat metabolism
They also act on the cardiovascular syslem. the skeletal muscles and the central nervous system.
- Effect on the inflammatory and immune process:
The anti-inflammatory, immunosuppressive and anti-allergic properties of glucocorticoids are responsible for most of the therapeutic applications These properties lead to the following results
- reduction of the immunoaclive cells near the inflammation focus,
- reduced vasodilation;
- stabilization of the lysosomal membranes.
- inhibition of phagocytosis:
- reduced production of prostaglandins and related substances
A dose of 4.4 mg methylprednisolone acetate (4 mg methylprednisolone) has the same glucocorticosteroid (anti-inflammatory) effect as 20 mg hydrocortisone Methylprednisolone has only a minimal mineralocorticoid effect (200 mg methylprednisolone are equivalent to 1 mg desoxycorticosterone)
-Effect on carbohydrate and protein metabolism.
Glucocorticoids have a protein calabolic action The liberated amino acids are converted into glucose and glycogen in the liver by means of the gluconeogenesis process Glucose absorption in peripheral tissues decreases, which can lead to hyperglycemia and glucosuremia. especially in patients who are prone to diabetes.
-Effect on fat metabolism
Glucocorticoids have a lipolytic action. This lipolytic activity mainly affects the limbs They also have a lipogenetic effect which is most evident on chest, neck and head. All this leads to a redistribution of the fat deposits
Maximum pharmacologic activity of glucocorticoids lays behind peak blood levels, suggesting that most effects ot the drugs result from modification
of enzyme activity rather than from direct actions by the drug
.
PHARMACOKINETICS
Methylprednisolone acetate is hydrolised to its active form by serum cholinesterases In man, methylprednisolone forms a weak dissociable bond with albumin and transcortin. Approximately 40 to 90% of the drug is bound The intracellular activity of glucocorticoids results in a clear difference between plasma half-life and pharmacological half-life Pharmacological activity persists after measurable plasma levels have disappeared. The duration of anti-inflammatory activity of glucocorticoids approximately equals the duration of hypothalamic-pituitary-adrenal (HPA) axis
suppression.
I.M. injections of 40 mg/ml give after approximately 7.3 ± 1 hour (Tmax) methylprednisolone serum peaks of 1.48 ± 0.86 ug/100 ml (Cmax). The half-life is in this case 69.3 hours. After a single I.M. injection of 40 to 80 mg methylprednisolone acetate, duration of HPA axis suppression ranged from 4 to 8 days.
An intra-articular injection of 40 mg in both knees (total dose: 80 mg) gives after 4 to 8 hours methylprednisolone peaks of approximately
21.5 ug/100 ml. After intra articular administration methylprednisolone acetate diffuses from the joint into systemic circulation over approximately
7 days, as demonstrated by the duration of the HPA axis suppression and by the serum methylprednisolone values.
Metabolism of methylprednisolone occurs via hepatic roules qualitatively similar to that of Cortisol. The major metabolites are 20 beta-
hydroxymethyl-prednisolone and 20 beta-hydroxy-6 alpha-methylprednisone. The metabolites are mainly excreted in the urine as glucuronides.
sulfates and unconjugated compounds. These conjugation reactions occur principally in the liver and to some extent in the kidney
Indications
Glucocorticoids should only be considered as symptomatic treatment, unless in case of some endocrine disorders, where they are used as a
substitution treatment
A. FOR INTRAMUSCULAR ADMINISTRATION Methylprednisolone acetate (DEPO-MEDROL) is not suitable tor the treatment of acute life threatening conditions If a rapid hormonal effect of maximum intensity is required, the IV administration of highly soluble methylprednisolone sodium succinate (SOLU-MEDROL) is indicated When oral therapy is not feasible and this preparation lend to the treatment of the condition, the intramuscular use of DEPO-MEDfiOL is indicated as follows
ANTI-INFAMMAT0RY TREATMENT
1 Rheumatic disorders ,
As adjuvant of a maintenance therapy (analgetics, kinesitherapy, tysiolherapy. etc) and for short-term administration (to tide the patient over an acute episode or exacerbation) in:
- psoriatic arthritis
- ankylosing spondylitis.
For the following indications, preference should be given to in situ administration if possible;
- post-traumatic osteoarthritis
-synovitis of osteoarthritis
- rheumatoid arthritis, including juvenile rheumatoid arthritis (selected cases may require low-dose maintenance therapy)
- acute and subacute bursitis
- epicondylitis
- acute nonspecilic tenosynovitis
- acute gouty arthritis.
2 Collagen diseases
During an exacerbation or as maintenance therapy in selected cases of:
- systemic lupus erythematosus
- systemic dermatomyositis (polymyositis)
- acute rheumatic carditis
3 Dermatologic diseases
- pemphigus
- severe erythema multiforme (Stevens-Johnson syndrome)
-exfoliative dermatitis
- mycosis lungoides ,
-bullous dermatitis herpetiformis (sulfone is the drug of first choice and systemic administration ot glucocorticoids is an adjuvant).
4 Allergic states
Control of severe or incapacitating allergic conditions intractable to adequate trials of conventional treatment in:
- chronic asthmatic respiratory disorders
- contact dermatitis
- atopic dermatitis
- serum sickness
- seasonal or perennial allergic rhinitis
-drug hypersensitivity reactions
- urticarial transfusion reactions
- acute noninfectious laryngeal edema (epinephrine is the drug of first choice).
5 Ophthalmic diseases
Severe acute and chronic allergic and inflammatory processes Involving the eye, such as:
- herpes zoster ophthalmicus
- iritis, iridocyclitis
- chorloretinitis
- diffuse posterior uveitis
- optic neuritis
6 Gastrointestinal diseases
To tide the patient over a critical period of the disease in:
- ulcerative colitis (systemic therapy)
- Crohn disease (systemic therapy).
7 Edematous states
To induces diuresis or remission of proteinuria in the nephrotic syndrome, without uremia, of of the idiopathic type or that due to lupus erythematosus.
8 Respiratory diseases
■ symptomatic pulmonary sarcoidosis berylliosis
■ fulminating or disseminated pulmonary tuberculosis when used concurrently with appropriate antitubercuious chemotherapy
■ Loefller's syndrome not manageable by other means
- aspiration pneumonitis
TREATMENT OF HEMATOLOGICAL AND ONCOLOGICAL DISORDERS
1 Hematologic disorders
-acquired ( auto immune) hemolytic anemia
- secondary thrombocytopenia in adults
■ erythroblastopenia (RBC anemia)
■ congenital (erythroid) hypoplastic anemia
2 Oncological diseases
For palliative management of
- leukemias and lymphomas
- acute leukemia of childhood
ENDOCRINE DISORDERS
- primary or secondary adrenocortical insufficiency
- acute adrenocortical insufficiency (hydrocortisone or cortisone is the drug of choice Synthetic analogues may be used in conjunction with mineralocorticoids where applicable; in infancy, mineralocorticoid supplementation is of particular importance.)
- congenital adrenal hyperplasia
- hypercalcemia associated wilh cancer
- nonsupporative thyroiditis
MISCELLANEOUS
- tuberculous meningitis with subarachnoid block or impending block when used concurrently with appropriate antitubercuious chemotherapy
- trichinosis with neurologic or myocardial involvement nervous system acute exacerbations of multiple sclerosis
B FOR INTRASYNOVIAL. PERIARTICULAR, INTRABURSAL OR SOFT TISSUE ADMINISTRATION (see also SPECIAL PRECAUTIONS)
DEPO-MEDROL is indicated as adjunctive therapy for short-term administration (to tide the patient over an acute episode or exacerbation) in;
- synovitis of osteoarthritis
- rheumatoid arthritis
- acute and subacute bursitis
- acute gouty arthritis
- epicondylitis
- acute nonspecific tenosynovitis
- post-traumatic osteoarthritis
C FOR INTRALESIONAL ADMINISTRATION
DEPO-MEDROL™ is indicated for intralesional use in the following conditions:
- keloids
- localized hypertropic. infiltraled, inflammatory lesions of lichen planus, psoriatic plaques, granuloma annulare and lichen simplex chronicus (neurodermatitis)
- discoid lupus erythematosus ,.,
- alopecia areata
DEPO-MEDROL may also be useful in cystic tumors or an aponeurosis or tendon (ganglia).
D FOR INTRARECTAL INSTILLATION
Ulcerative colitis.
Dosage and administration
A I.M. ADMINISTRATION FOR SYSTEMIC EFFECT
The intramuscular dosage will vary with the condition being treated When a prolonged effect is desired, the weekly dose may be calculated by multiplying the daily oral dose by 7 and given as a singular intramuscular injection
Dosage must be individualized according to the severity of the disease and response of the patient In general, the duration of the treatment should he kept as short as possible Medical surveillance is necessary
For infants and children, the recommended dosage will have to be reduced, but dosage should be governed by the severity of the condition rather than by strict adherence to the ratio indicated by age or body weight
Hormone therapy is adjunct to and not a replacement for conventional therapy. Dosage must be decreased or discontinued gradually when the drug has been administered for more than a few days Severe medical surveillance is recommended when a chronic treatment is discontinued The severity, prognosis and expected duration ot the disease and the reaction of the patient to medication are primary factors in determining dosage. a period of spontaneous remission occurs in a chronic condition, treatment should be discontinued. Routine laboratory studies, such as urinalysis, two-hour postprandial blood sugar, determination of blood pressure and body weight and a chest X-ray should be made at regular intervals during prolonged therapy. Upper GI X-rays are desirable in patients with an ulcer history or significant dyspepsia In patients with the adrenogenital syndrome, a single intramuscular injection of 40 mg every two weeks may be adequate. For maintenance of patients with rheumatoid arthritis, the weekly intramuscular dose will vary from 40 to 120 mg The usual dosage for patients wilh dermalologic lesions benefited by systemic corticoid therapy is 40 to 120 mg of methylptedmsolone acetate administered intramuscularly at weekly intervals for one to four weeks. In acute severe dermatitis due to poison ivy. relief may result within 8 to 12 hours following intramuscular administration of a single dose of 80 to 120 mg. In chronic contact dermatitis repeated injections at 5 to 10 day intervals may be necessary. In seborrheic dermatitis, a weekly dose of 80 mg may be adequate to control the condition Following intramuscular administration of 80 to 120 mg to asthmatic patients, relief may result within 6 to 48 hours and persist for several days to two weeks.
Similarly in patients with allergic rhinitis (hay fever) an intramuscular dose of 80 to 120 mg may be followed by relief of coryzal symptoms within six hours persisting for several days to three weeks.
If signs of stress are associated with the condition being treated, the dosage of the suspension should be increased If a rapid hormonal effect of maximum intensity is required, the intravenous administration of highly soluble methylpredmsolone sodium succinate is indicated.
B. IN SITU ADMINISTRATION FOR LOCAL EFFECT
Therapy with DEPO-MEDROL does not obviate the need for the conventional measures usually employed. Although this method ot treatment will ameliorate symptoms, it is in no sense a cure and the hormone has no effect on the cause of the inflammation
1 Rheumatoid and osteoarthritis
The dose for intra-articular administration depends upon the size of the joint and varies with the severity of the condition in the individual patient. In chronic cases, several injections can vary from one to five per week, depending on the degree of relief obtained from the initial injection The doses in the following table are given as a general guide:
| Size of joint | Eamples | Range of dosage |
| Large | Knees Ankles Shoulders | 20 to 80 mg |
| Medium | Elbows Wrists | 10 to 40 mg |
| Small | Metacarpophalangeal Inlerphalangeal Sternoclavicular Acromioclavicular | 4 to 10 mg |
Procedure; It is recommended that the anatomy of the joint involved be reviewed before attempting intraarticular injection In order to obtain the full anti-inflammatory effect it is important that the injection be made into the synovial space Employing the same sterile technique as for a lumbar puncture, a sterile 20 to 24 gauge needle (on a dry syringe) is quickly inserted into the synovial cavity Procaine infiltration is elective. The aspiration of only a few drops of joint fluid proves the joint space has been entered by the needle The injection site for each joint is determined by that location where the synovial cavity is most superficial and most free of large vessels and nerves With the needle in place, the aspirating syringe is removed and replaced by a second syringe containing the desired amount of DEP0-MEDROL The plunger is then pulled outward slightly to aspirate synovial fluid and to make sure the needle is still in the synovial space After injection. the joint is moved gently a few times to aid mixing of the synovial fluid and the suspension The site is covered with a small sterile dressing. Suitable sites for intra-articular injection are the knee, ankle, wrist, elbow, shoulder, phalangeal and hip joints Since difficulty is occasionally encountered in entering the hip joint, precautions should be taken to avoid any large blood vessels in the area Joints not suitable for injection are those that are anatomically inaccessible such as the spinal joints and those like the sacroiliac joints that are devoid of synovial space Treatment failures are most frequently the result of failure to enter the joint space Little or no benefit follows injection into surrounding tissue If failures occur when injections into the synovial spaces are certain, as determined by aspiration of fluid, repeated injections are usually futile. Local therapy does not alter the underlying disease process, and whenever possible comprehensive therapy including physiotherapy and orthopedic correction should be employed
2, Bursitis
The area around the injection site is prepared in a sterile way and a wheal at the site made with 1% procaine hydrochloride solution. A 20 to 24 gauge needle attached to a dry syringe is inserted into the bursa and the fluid aspirated The needle is left in place and the aspirating syringe changed tor a small syringe containing the desired dose After injection, the needle is withdrawn and a small dressing applied
3 Miscellaneous; ganglion, tendinitis, epicondylitis
In the trealment of conditions such as tendinitis or tenosynovitis, care should be taken to inject the suspension into the tendon sheath rather than into the substance of the tendon The tendon may be readily palpated when placed on a stretch When treating conditions such as epicondylitis, the area of greatest tenderness should be outlined carefully and the suspension infiltrated into the area, for ganglia of the tendon sheaths, the suspension is injected directly into the cyst
In many cases, a single infection causes a marked decrease in the size of the cystic tumor and may effect disappearance.
The usual sterile precautions should be observed, of course, with each injection (application of a suitable antiseptic to the skin)
The dose in the treatment of the various conditions of the tendinous or bursal structures listed above varies with the condition being treated and
ranges from 4 to 30 mg. In recurrent or chronic conditions, repeated injections may be necessary
4 Injections for local effect in dermalologic conditions
Following cleansing with an appropriate antiseptic such as 70% alcohol, 20 to 60 mg oi the suspension is injected into the lesion. It may be necessary to distribute doses ranging from 20 to 40 mg by repeated local injections in the case of large lesions. Care should be taken to avoid injection of sufficient material to cause blanching since this may be followed by a small slough One to four injections are usually employed, the intervals between injections varying with the type of lesion being treated and the duration of improvement produced by the initial injection
C INTRARECTAL ADMINISTRATION
DEPO-MEDROL™ in doses of 40 to 120 mg administered as retention enemas or by continuous drip three to seven times weekly for periods of two or more weeks, have been shown to be a useful adjunct in the trealment ot some patients with ulcerative colitis Many patients can be controlled with 40 mg of DEPO-MEDROL administered in from 30 to 300 ml of water Other accepted therapeutic measures snould, of course, be instituted
INSTRUCTIONS FOR USE
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration A strict sterile technique is needed in order to prevent iatrogen infections. This product is not suitable for IV and intrathecal administration and may not be used as a multidose vial Following administration of the desired dose, any remaining suspension should be discarded
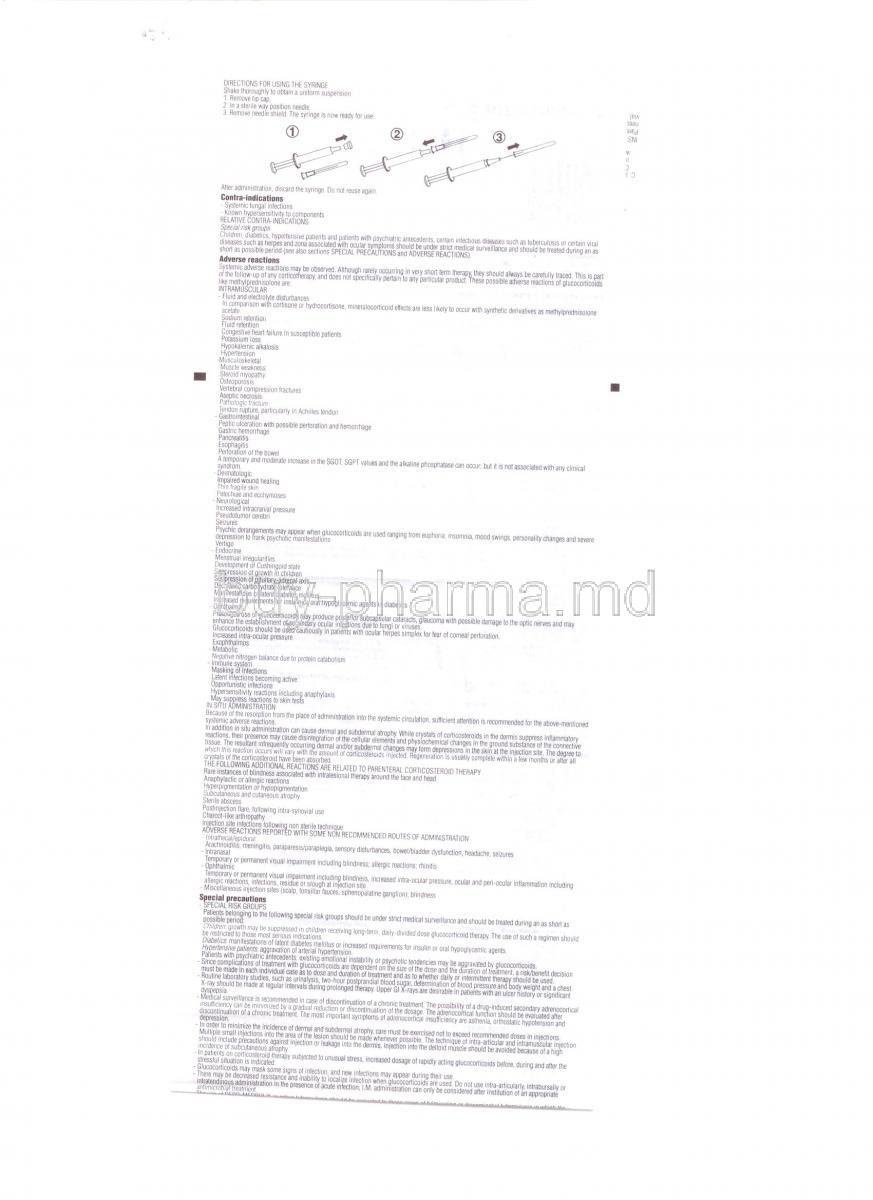
DIRECTIONS FOR USING THE SYRINGE
Shake thoroughly to obtain a uniform suspension.
1. Remove tip cap.
2. In a sterile way position needle.
3. Remove needle shield. The syringe is now ready for use.
After administration, discard the syringe. Do not reuse again.
Contraindications
- Systemic fungal infections
- Known hypersensitivity to components RELATIVE CONTRA-INDICATIONS
Special risk groups
Children, diabetics, hypertensive patients and patients with psychiatric antecedents, certain infectious diseases such as tuberculosis or certain viral diseases such as herpes and zona associated with ocular symptoms should be under strict medical surveillance and should be treated during an as short as possible period (see also sections SPECIAL PRECAUTIONS and ADVERSE REACTIONS). Adverse reactions
Systemic adverse reactions may be observed. Although rarely occurring in very short term therapy, they should always be carefully traced. This is part of the follow-up of any corticotherapy. and does not specifically pertain to any particular product These possible adverse reactions of glucocorticoids like methylprednisolone are:
INTRAMUSCULAR
- Fluid and electrolyte disturbances
In comparison with cortisone or hydrocortisone, mineralocorticoid effects are less likely to occur with synthetic derivatives as methylprednisolone
acetate
Sodium retention
Fluid retention
Congestive heart failure in susceptible patients
Potassium loss
Hypokalemic alkalosis
Hypertension -
Musculoskeletal
Muscle weakness
Steroid myopathy
Osteoporosis
Vertebral compression fractures
Aseptic necrosis
Pathologic fracture
Tendon rupture, particular in Achilles tendon
Gastrointestinal
Peptic ulceration with possible perforation and hemorrhage
Gastric hemorrhage
Pancreatitis
Escphagifis
Perforation of the bowel
A temporary and moderate increase in the SG0T, SGPT values and the alkaline phosphatase can occur; but it is not associated with any clinical syndrom.
- Dermatologic
Impaired wound healing
Thin fragile skin
Petechiae and ecchymoses
- Neurological
Increased intracranial pressure
Pseudotumor cerebri
Seizures
Psychic derangements may appear when glucocorticoids are used ranging from euphoria, insomnia, mood swings, personality changes and severe
depression to frank psychotic manifestations
Vertigo
- Endocrine
Menstrual irregularities
Development of Cushingoid state Suppression of growth in children
Suppression ot pituitary-adrenal axis
Decreased carbohydrate tolerance
Manifestations of latent diabetes mellitus
Increased requirements for insulin or oral hypoglycemic agents in diabetics
- Ophthalmic
Prolonged use of glucocorticoids may produce posterior subcapsular cataracts, glaucoma with possible damage to the optic nerves and may
enhance the establishment of secondary ocular infections due to fungi or viruses.
Glucocorticoids should be used cautiously in patients with ocular herpes simplex for fear of corneal perforation.
Increased intra-ocular pressure
Exophthalmos
- Metabolic
Negative nitrogen balance due to prolein catabolism
- Immune system
Masking of infections
Latent infections becoming active
Opportunistic infections
Hypersensitivity reactions including anaphylaxis
May suppress reactions to skin tests
in situ Administration
Because of the resorption from the place of administration into the systemic circulation, sufficient attention is recommended for the above-mentioned systemic adverse reactions.
In addition in situ administration can cause dermal and subdermal atrophy While crystals of corticosteroids in the dermis suppress inflammatory reactions, their presence may cause disintegration of the cellular elements and physiochemical changes in the ground substance of the connective tissue. The resultant infrequently occurring dermal and/or subdermal changes may form depressions in the skin at the injection site The degree to which this reaction occurs will vary with the amount of corticosteroids injected Regeneration is usually complete within a few months or after all crystals of the corticosteroid have been absorbed.
THE FOLLOWING ADDITIONAL REACTIONS ARE RELATED TO PARENTERAL CORTICOSTEROID THERAPY Rare instances of blindness associated with intralesional therapy around the lace and head
Anaphylactic or allergic reactions
Hyperpigmentation or hypopigmentalion
Subcutaneous and cutaneous atrophy
Sterile abscess
Postinjection flare, following intra-synovial use
Charcot-like arthropathy
Injection site infections following non sterile technique
ADVERSE REACTIONS REPORTED WITH SOME NON RECOMMENDED ROUTES OF ADMINISTRATION
- Intrathecal/epidural
Arachnoiditis, meningitis, paraparesis/paraplegia, sensory disturbances, bowel/bladder dysfunction, headache, seizures
- Intranasal
Temporary or permanent visual impairment including blindness, allergic reactions; rhinitis
- Ophthalmic
Temporary or permanent visual impairment including blindness, increased intra-ocular pressure, ocular and peri-ocular inflammation including allergic reactions, infections, residue or slough at injection site
- Miscellaneous injection sites (scalp, tonsillar fauces, sphenopalatine ganglion): blindness Special precautions
- SPECIAL RISK GROUPS
Patients belonging to the following special risk groups should be under strict medical surveillance and should be treated during an as short as possible period:
Children: growth may be suppressed in children receiving long-term, daily-divided dose glucocorticoid therapy. The use of such a regimen should be restricted to those most serious indications.
Diabetics, manifestations of latent diabetes mellitus or increased requirements for insulin or oral hypoglycemic agents. Hypertensive patients aggravation of arterial hypertension.
Patients with psychiatric antecedents: existing emotional instability or psychotic tendencies may be aggravated by glucocorticoids,
- Since complications of treatment with glucocorticoids are dependent on the size of the dose and the duration of treatment, a risk/benefit decision must be made in each individual case as to dose and duration of treatment and as to whether daily or intermittent therapy should be used.
- Routine laboratory studies, such as urinalysis, two-hour postprandial blood sugar, determination of blood pressure and body weight and a chest X-ray should be made at regular intervals during prolonged therapy Upper Gl X-rays are desirable in patients with an ulcer history or significant dyspepsia
- Medical surveillance is recommended in case of discontinuation of a chronic treatment. The possibility of a drug-induced secondary adrenocortical insufficiency can be minimized by a gradual reduction or discontinuation of the dosage The adrenocortical function should be evaluated after discontinuation of a chronic treatment. The most important symptoms of adrenocortical insufficiency are asthenia, orthostatic hypotension and depression
- In order to minimize the incidence of dermal and subdermal atrophy, care must be exercised not to exceed recommended doses in injections. Multiple small injections into the area of the lesion should be made whenever possible The technique of intra-articular and intramuscular injection should include precautions against injection or leakage into the dermis. Injection into the deltoid muscle should be avoided because of a high incidence of subcutaneous atrophy.
- In patients on corticosteroid therapy subjected to unusual stress, increased dosage of rapidly acting glucocorticoids before, during and after the antimicrobral treatment.
- The use of DEPO-MEDROL in active tuberculosis should be restricted to those cases of fulminating or disseminated tuberculosis in which the corticosteroid is used (or the management ot the disease in conjunction with appropriate antituberculosis regimen, If glucocorticoids are indicated in patients with latent tuberculosis or tuberculin reactivity, close observation is necessary as reactivation of the disease may occur. During prolonged corticosteroid therapy, these patients should receive chemoprophylaxis.
- Because rare instances of anaphylactic reactions have occurred in patients receiving parenteral corticosteroid therapy, appropriate precautionary measuies should be taken prior to administration, especially when the patient has a history of allergy to any drug.
- Allergic skin reactions have been reported apparently related to the excipients Rarely has skin testing demonstrated a reaction to methylprednisolone acetate, per se
- Glucocorticoids should be used with caution in non specific ulcerative colitis, it there is a probability of impending perforation, abscess or other pyogenic infection. Caution must also be used in diverticulitis, fresh intestinal anastomoses, active or latent peptic ulcer, renal insufficiency, hypertension, osteoporosis and myasthenia gravis, when steroids are used as direct or adjunctive therapy
- No evidence exists showing that glucocorticoids are carcinogenic, mutagenic or impair fertility.
- Corticotherapy has to be considered when interpreting a whole series of biological tests and parameters (e g skin tests, thyroid hormone levels)
INTRA-ARTICULAR USE
In case of mtra-articular use and/or other local administration a strict sterile technique is needed to avoid latrogen infections. Following intra-articular corticosteroid therapy, care should be taken to avoid overuse of joints in which symptomatic benefit has been obtained. Negligence in this matter may permit an increase in joint deterioration that will more than offset the beneficial effects of the steroid. Unstable joints should not be injected Repeated intra-articular injection may in some cases result in instability of the joint X-ray follow-up is suggested in selected cases to detect deterioration If a local anesthetic is used prior to injection of DEPO-MEDROL, the anesthetic package insert should be read carefully and all the precautions observed.
THE FOLLOWING ADDITIONAL PRECAUTIONS APPLY FOR PARENTERAL GLUCOCORTICOIDS
- Intrasynovial injection of a corticosteroid may produce systemic as well as local effects
- Appropriate examination of any joint fluid present is necessary to exclude a septic process.
- A marked increase in pain accompanied by local swelling, further restriction of joint motion, lever and malaise are suggestive of septic arthritis If this complication occurs and the diagnosis of sepsis is confirmed. local injections of glucocorticoids should be discontinued and appropriate antimicrobial therapy should be instituted.
- Local injection of a steroid into a previously infected joint is to be avoided
- Glucocorticoids should not be injected into unstable joints. Sterile technique is necessary to prevent infections or contamination.
- Although controlled clinical trials have shown glucocorticoids to be effective in speeding the resolution of acute exacerbations of multiple sclerosis, they do not show that glucocorticoids affect the ultimate outcome or natural history of the disease. The studies do show that relatively high doses of glucocorticoids are necessary to demonstrate a significant effect.
Incompatibilities
Because of possible physical incompatibilities DEPO-MEDROL should not be diluted or mixed with other solutions.
Pregnancy and lactation
Some animal studies have shown that corticosteroids when administered to the mother at high doses may cause fetal malformations.
Since adequate human reproduction studies have not been done with glucocorticoids, the use of these drugs in pregnancy, nursing mothers or
women of childbearing potential, requires that the possible benefits of the drug be weighed against the potential hazards to the mother and embryo or
fetus.
Glucocorticoids should be used during pregnancy only if clearly needed If a chronic treatment with corticosteroids has to be stopped during pregnancy (as with other chronic treatments), this should occur gradually (see also DOSAGE AND ADMINISTRATION). In some cases (e.g. substitution treatment of adrenocortical insufficiency) however it can be necessary to continue treatment or even to increase dosage Corticosteroids readily cross the placenta
New-born infants born of mothers who have received substantial doses of glucocorticosteroids during pregnancy, should be carefully observed and
evaluated for signs of adrenal insufficiency.
In case of labor and delivery no effects are known.
Corticosteroids are excreted in breast milk.
Interactions
DESIRED INTERACTIONS
- By the treatment of fulminating or disseminated pulmonary tuberculosis and tuberculous meningitis with subarachnoid block or impending block, methylprednisolone is used concurrently with appropriate antituberculous chemotherapy
- By the treatment of neoplastic diseases like leukemia and lymphoma, methylprednisolone is usually used m conjunction with an alkylating agent, an antimetabolite and a vinca alkaloid.
UNDESIRED INTERACTIONS
- Glucocorticoids may increase renal clearance of salicylates This could lead to a decrease in salicylate serum levels and to salicylate toxicity when the administration of corticoids is stopped.
- Drugs such as troleandomycm and ketoconazole may inhibit the metabolism of corticoids. An adaptation of the corticoid dose may be required in order to avoid an overdosage
- Concurrent administration of barbiturates, phenylbutazone, phenytom or rifampicm may enhance the metabolism and reduce the effects of corticoids.
- Response to anticoagulants can both be reduced and increased by corticoids. Therefore coagulation should be monitored.
- While on corticosteroid therapy patients should not be vaccinated against smallpox Other immunization procedures should not be undertaken in patients who are on glucocorticoids, especially on high doses because of possible hazards of neurological complications and lack of antibody response
Glucocorticoids may increase the requirements for insulin or oral hypoglycemic agents in diabetics Combination of glucocorticosteroids with thiazid-diuretics increases the risk of glucose intolerance
- Concurrent use ot ulcerogenic drugs (eg salicylates. NSAI drugs) may increase the risk of gastrointestinal ulceration
- Acetylsalicylic acid should be used cautiously m conjunction with glucocorticoids in hypoprothrombinemia
- Convulsions have been reported with concurrent use of methylpreonisone and cyclosporin Mutual inhibition of metabolism occurs with concurrent use of these two products Therefore it is possible that convulsions and other adverse reactions associated with the individual use of these drugs may be more apt to occur.
Ability to drive and to operate machinery
Although visual disorders belong to the rare adverse reactions, caution is recommended by patients driving cars and/or using machines
Overdosage
There is no clinical syndrome of acute overdosage with methylprednisolone acetate.
Repeated frequent doses (daily or several times per week) over a protracted period may result in a Cushingoid state.
Storage
Store at controlled room temperature (20°-25°C). Manufacturer: Pfizer Manufacturing Belgium NV Rijksweg 12,2870 Puurs Belgium
(C) Copyright Pharmacia 95A30
CPS24I93
Marketed by:
Pfizer Products India Private Limited 5 Patel Estate, S.V. Road, Jogeshwari (W), Mumbai 400102 INDIA
5R8183